The Cause Of Bunions?
Overview
 A bunion is an enlargement of ?the metatarsophalangeal (MTP) joint?, this is the big toe?s base joint that forms when the bone or tissue moves out of place. This forces the toe to bend toward the others, causing an often painful lump of bone on the foot. The MTP joint, which carries lots of weight, is stiff and sore, making even the wearing of shoes difficult or impossible. It also causes swelling of the feet to occur. Hammer toes are also associated with the formation of bunions.
A bunion is an enlargement of ?the metatarsophalangeal (MTP) joint?, this is the big toe?s base joint that forms when the bone or tissue moves out of place. This forces the toe to bend toward the others, causing an often painful lump of bone on the foot. The MTP joint, which carries lots of weight, is stiff and sore, making even the wearing of shoes difficult or impossible. It also causes swelling of the feet to occur. Hammer toes are also associated with the formation of bunions.
Causes
High heels can exacerbate a potential bunion problem because they tip the body?s weight forward, forcing the toes into the front of the shoe. This may help to explain why bunions are 10 times more common in women than in men. People in occupations such as teaching and nursing, that involve a lot of standing and walking, are susceptible to bunions. Ballet dancers, whose feet suffer severe repetitive stress, are also amongst those who experience bunions. Women can sometimes develop bunions and other foot problems during pregnancy because hormonal changes loosen the ligaments and flatten the feet. Bunions are also associated with arthritis, which damages the cartilage within the joint.
Symptoms
Red, thickened skin along the inside edge of the big toe. A bony bump at this site. Pain over the joint, which pressure from shoes makes worse. Big toe turned toward the other toes and may cross over the second toe.
Diagnosis
Before examining your foot, the doctor will ask you about the types of shoes you wear and how often you wear them. He or she also will ask if anyone else in your family has had bunions or if you have had any previous injury to the foot. In most cases, your doctor can diagnose a bunion just by examining your foot. During this exam, you will be asked to move your big toe up and down to see if you can move it as much as you should be able to. The doctor also will look for signs of redness and swelling and ask if the area is painful. Your doctor may want to order X-rays of the foot to check for other causes of pain, to determine whether there is significant arthritis and to see if the bones are aligned properly.
Non Surgical Treatment
Bunions can be treated conservatively (without surgery) using simple measures such as well-fitting shoes, orthoses simple painkillers and padding. Physiotherapy can help improve associated muscle imbalances. Such measures will not correct or even stop the deformity but they can help with symptoms. When non-surgical treatments prove insufficient, surgery can relieve your pain, correct any related foot deformity and help you resume your normal activities. 
Surgical Treatment
Research shows that 85% of people who have bunion corrections are satisfied with the results. However, a number of problems can arise. The big toe is usually stiffer than before. For most people this does not matter, but for athletes or dancers it is very important. As mentioned before, the big toe is slightly weaker with a bunion, and this transfers weight onto the ball of the foot. After bunion surgery, this transfer of weight can increase. Therefore, if you have pain under the ball of the foot ("metatarsalgia") it may be worse after bunion surgery, and it may also develop for the first time. Careful surgical technique can reduce this risk, but it cannot avoid it completely. Most people who develop metatarsalgia are comfortable with a simple insole in the shoe but occasionally surgery is required. In some people the big toe slowly tilts back toward the original position and occasionally this is bad enough to need to have the operation redone. On the other hand, the toe can tilt the other way, though much more rarely. Again, occasionally this is bad enough to need to have the operation redone. Infections in the wound, plaster problems and minor damage to the nerves of the toe can occur in any foot surgery. Usually these are minor problems that get better quickly. This may sound like a lot of possible problems, but in fact most people do not get them and are satisfied with their bunion surgery. However, this may help you to see how important it is to have any bunion surgery carried out by a properly trained and experienced foot and ankle surgeon.
Prevention
The best protection against developing bunions is to protect and care for your feet every day. Avoid tight and narrow-fitting shoes. Limit your use of high heels. Wear comfortable shoes with adequate space between your longest toe and the end of the shoe. Getting treatment for very flat or very high-arched feet (if you are experiencing symptoms) will give your feet the proper support and help maintain stability and balance.
Discover More About Over-Pronation
Overview
One of the main postural deviations that cause pain and injury in the foot and ankle area (and resultant compensations in the rest of the body) is overpronation. Pronation is a normal function that occurs when the foot rolls inward toward the midline of the body. This movement causes the heel to collapse inward and the medial arch of the foot to elongate and flatten. Overpronation, however, is when the foot collapses too far inward for normal function. Consequently, this directly affects the ability of the foot to perform and can disrupt proper functioning through the entire body.
Causes
There is a relationship between biomechanics and injury that is specific to each body part. Overall though, poor mechanics will either increase the landing forces acting on the body or increase the work to be done by the muscles. Both increase the stress, which, depending on the individual and the amount of running can become excessive and cause injury.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
Over-pronation and the problems that go with it are treated with shoe inserts called arch supports or orthotics. You can buy orthotics at a pharmacy or athletic shoe store or they can be custom made. Make sure the arch supports are firm. If you can easily bend them in half, they may be too flexible.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
One of the main postural deviations that cause pain and injury in the foot and ankle area (and resultant compensations in the rest of the body) is overpronation. Pronation is a normal function that occurs when the foot rolls inward toward the midline of the body. This movement causes the heel to collapse inward and the medial arch of the foot to elongate and flatten. Overpronation, however, is when the foot collapses too far inward for normal function. Consequently, this directly affects the ability of the foot to perform and can disrupt proper functioning through the entire body.
Causes
There is a relationship between biomechanics and injury that is specific to each body part. Overall though, poor mechanics will either increase the landing forces acting on the body or increase the work to be done by the muscles. Both increase the stress, which, depending on the individual and the amount of running can become excessive and cause injury.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
Over-pronation and the problems that go with it are treated with shoe inserts called arch supports or orthotics. You can buy orthotics at a pharmacy or athletic shoe store or they can be custom made. Make sure the arch supports are firm. If you can easily bend them in half, they may be too flexible.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
What Are The Causes Of Calcaneal Apophysitis?
Overview
A syndrome of heel pain in skeletally immature individuals. The formal name is: calcaneal apophysitis. The pain is thought to arise from the growth plate (apophysis) and epiphysis. It is thought to be an overuse phenomena. Overloading of the apophysis by both traction (due to Achilles tendon) and compression (sue to weightbearing) have been implicated. Reversible pathologic alterations occur in the apophysis, which cause secondary pain. It is the growth plate and its bone, at the back of the heel bone (calcaneus), whose presence allows for longitudinal growth of calcaneus.
Causes
The cause of Sever's disease is not entirely clear. It is most likely due to overuse or repeated minor trauma that happens in a lot of sporting activities - the cartilage join between the two parts of the bone can not take all the shear stress of the activities. Some children seem to be just more prone to it for an unknown reason - combine this with sport, especially if its on a hard surface and the risk of getting it increases. It can be almost epidemic at the start of some sports seasons, especially winter. At the start of winter, the grounds are often harder, but soften later. Children who are heavier are also at greater risk for developing calcaneal apophysitis.
Symptoms
On examination, the typical signs are tenderness on palpation of the heel, particularly on deep palpation at the Achilles tendon insertion. Pain on dorsiflexion of the ankle, particularly when doing active toe raises; forced dorsiflexion of the ankle is also uncomfortable. Swelling of the heel, usually mild. Calcaneal enlargement, in long-standing cases.
Diagnosis
Sever's disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order X-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
The disease itself is self limiting and will resolve regardless of treatment once the growth plate has fully closed. Depending on the age of the youth at onset this could be a problem for many years. Treatment has always been aimed at managing the pain as well as the inflammation. This is done with the rest, ice, non steroidal anti-inflammatories like ibuprofen, stretching, taping, heel cups, heel lifts and orthotics. In severe cases, cast or walking boot immobilization is used. Each of these have differing levels of efficacy but in my experience orthotics are the golden treatment or the silver bullet. I am not talking about your run of the mill over the counter Dr. Scholls shoe insert. These definitely have their place in the world but not here. Custom molded orthotics made from a mold taken of the youths foot will provide the necessary control and support to stop the pain cycle. We can safely report over 85% of patients who are able to get back to sports and other activities as long as they wear the orthotics in supportive shoes as directed.
Recovery
Severs disease is a self limiting condition that gradually resolves as the patient moves towards skeletal maturity. This usually takes between 6 to 12 months, but may persist for as long as 2 years. With appropriate management, symptoms may resolve in a number of weeks. Patients with Severs disease typically improve gradually over time and full function is restored.
A syndrome of heel pain in skeletally immature individuals. The formal name is: calcaneal apophysitis. The pain is thought to arise from the growth plate (apophysis) and epiphysis. It is thought to be an overuse phenomena. Overloading of the apophysis by both traction (due to Achilles tendon) and compression (sue to weightbearing) have been implicated. Reversible pathologic alterations occur in the apophysis, which cause secondary pain. It is the growth plate and its bone, at the back of the heel bone (calcaneus), whose presence allows for longitudinal growth of calcaneus.
Causes
The cause of Sever's disease is not entirely clear. It is most likely due to overuse or repeated minor trauma that happens in a lot of sporting activities - the cartilage join between the two parts of the bone can not take all the shear stress of the activities. Some children seem to be just more prone to it for an unknown reason - combine this with sport, especially if its on a hard surface and the risk of getting it increases. It can be almost epidemic at the start of some sports seasons, especially winter. At the start of winter, the grounds are often harder, but soften later. Children who are heavier are also at greater risk for developing calcaneal apophysitis.
Symptoms
On examination, the typical signs are tenderness on palpation of the heel, particularly on deep palpation at the Achilles tendon insertion. Pain on dorsiflexion of the ankle, particularly when doing active toe raises; forced dorsiflexion of the ankle is also uncomfortable. Swelling of the heel, usually mild. Calcaneal enlargement, in long-standing cases.
Diagnosis
Sever's disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order X-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
The disease itself is self limiting and will resolve regardless of treatment once the growth plate has fully closed. Depending on the age of the youth at onset this could be a problem for many years. Treatment has always been aimed at managing the pain as well as the inflammation. This is done with the rest, ice, non steroidal anti-inflammatories like ibuprofen, stretching, taping, heel cups, heel lifts and orthotics. In severe cases, cast or walking boot immobilization is used. Each of these have differing levels of efficacy but in my experience orthotics are the golden treatment or the silver bullet. I am not talking about your run of the mill over the counter Dr. Scholls shoe insert. These definitely have their place in the world but not here. Custom molded orthotics made from a mold taken of the youths foot will provide the necessary control and support to stop the pain cycle. We can safely report over 85% of patients who are able to get back to sports and other activities as long as they wear the orthotics in supportive shoes as directed.
Recovery
Severs disease is a self limiting condition that gradually resolves as the patient moves towards skeletal maturity. This usually takes between 6 to 12 months, but may persist for as long as 2 years. With appropriate management, symptoms may resolve in a number of weeks. Patients with Severs disease typically improve gradually over time and full function is restored.
Achilles Tendon Surgery Exercises
Overview
 Achilles Tendon Rupture Surgery is a surgical procedure is used to repair a ruptured Achilles tendon. There are two types of surgery an open surgery and a percutaneous surgery, in both cases the surgeon sews the tendon back together through the incision helping the tendon to heal properly and restore function to the foot and ankle. If the injury or rupture has caused severe swelling the surgery may be delayed for a short period of time to allow the swelling to go down.
Achilles Tendon Rupture Surgery is a surgical procedure is used to repair a ruptured Achilles tendon. There are two types of surgery an open surgery and a percutaneous surgery, in both cases the surgeon sews the tendon back together through the incision helping the tendon to heal properly and restore function to the foot and ankle. If the injury or rupture has caused severe swelling the surgery may be delayed for a short period of time to allow the swelling to go down.
Causes
The tendon usually ruptures without any warning. It is most common in men between the ages of 40-50, who play sports intermittently, such as badminton and squash. There was probably some degeneration in the tendon before the rupture which may or may not have been causing symptoms.
Symptoms
Patients with an Achilles tendon rupture frequently present with complaints of a sudden snap in the lower calf associated with acute, severe pain. The patient reports feeling like he or she has been shot, kicked, or cut in the back of the leg, which may result in an inability to ambulate further. A patient with Achilles tendon rupture will be unable to stand on his or her toes on the affected side.
Diagnosis
Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis.
Non Surgical Treatment
Once a diagnosis of Achilles tendon rupture has been confirmed, a referral to an orthopaedic specialist for treatment will be recommended. Treatment for an Achilles tendon rupture aims to facilitate the torn ends of the tendon healing back together again. Treatment may be non-surgical (conservative) or surgical. Factors such as the site and extent of the rupture, the time since the rupture occurred and the preferences of the specialist and patient will be considered when deciding which treatment will be undertaken. Some cases of rupture that have not responded well to non-surgical treatment may require surgery at a later stage. The doctor will immobilise the ankle in a cast or a special hinged splint (known as a ?moon boot?) with the foot in a toes-pointed position. The cast or splint will stay in place for 6 - 8 weeks. The cast will be checked and may be changed during this time. 
Surgical Treatment
Some surgeons feel an early surgical repair of the tendon is beneficial. The surgical option was long thought to offer a significantly smaller risk of re-rupture compared to traditional non-operative management (5% vs 15%). Of course, surgery imposes higher relative risks of perioperative mortality and morbidity e.g. infection including MRSA, bleeding, deep vein thrombosis, lingering anesthesia effects, etc.
Prevention
The best treatment of Achilles tendonitis is prevention. Stretching the Achilles tendon before exercise, even at the start of the day, will help to maintain ankle flexibility. Problems with foot mechanics can also lead to Achilles tendonitis. This can often be treated with devices inserted into the shoes such as heel cups, arch supports, and custom orthotics.
How Does Leg Length Discrepancy Have An Affect On Gait
Overview
Have you ever been told or noticed that one of your legs is a bit longer than the other? Do you have incidences of lower back pain? These two things could be related. Most individuals have a small difference in their leg lengths. For some, the discrepancy is small and negligible and will not be a contributor to lower back pain. This is usually the case for people if their leg length is less than 5 millimeters. However, a difference of leg lengths greater than 5 millimeters (1/4 inch) can contribute to lower back pain. If you have a leg length difference of greater than 9 mm, then you have a 6X greater likelihood of having an episode of lower back pain.
Causes
There are many causes of leg length discrepancy. Structural inequality is due to interference of normal bone growth of the lower extremity, which can occur from trauma or infection in a child. Functional inequality has many causes, including Poliomyelitis or other paralytic deformities can retard bone growth in children. Contracture of the Iliotibial band. Scoliosis or curvature of the spine. Fixed pelvic obliquity. Abduction or flexion contraction of the hip. Flexion contractures or other deformities of the knee. Foot deformities.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
You and your physician should discuss whether treatment is necessary. For minor LLDs in adults with no deformity, treatment may not be necessary. Because the risks may outweigh the benefits, surgical treatment to equalize leg lengths is usually not recommended if the difference is less than one inch. For these small differences, your physician may recommend a shoe lift. A lift fitted to the shoe can often improve your walking and running, as well as relieve back pain caused by LLD. Shoe lifts are inexpensive and can be removed if they are not effective. They do, however, add weight and stiffness to the shoe.

Surgical Treatment
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
Have you ever been told or noticed that one of your legs is a bit longer than the other? Do you have incidences of lower back pain? These two things could be related. Most individuals have a small difference in their leg lengths. For some, the discrepancy is small and negligible and will not be a contributor to lower back pain. This is usually the case for people if their leg length is less than 5 millimeters. However, a difference of leg lengths greater than 5 millimeters (1/4 inch) can contribute to lower back pain. If you have a leg length difference of greater than 9 mm, then you have a 6X greater likelihood of having an episode of lower back pain.
Causes
There are many causes of leg length discrepancy. Structural inequality is due to interference of normal bone growth of the lower extremity, which can occur from trauma or infection in a child. Functional inequality has many causes, including Poliomyelitis or other paralytic deformities can retard bone growth in children. Contracture of the Iliotibial band. Scoliosis or curvature of the spine. Fixed pelvic obliquity. Abduction or flexion contraction of the hip. Flexion contractures or other deformities of the knee. Foot deformities.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
You and your physician should discuss whether treatment is necessary. For minor LLDs in adults with no deformity, treatment may not be necessary. Because the risks may outweigh the benefits, surgical treatment to equalize leg lengths is usually not recommended if the difference is less than one inch. For these small differences, your physician may recommend a shoe lift. A lift fitted to the shoe can often improve your walking and running, as well as relieve back pain caused by LLD. Shoe lifts are inexpensive and can be removed if they are not effective. They do, however, add weight and stiffness to the shoe.
Surgical Treatment
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
Acquired Flat Foot
Overview
A variety of foot problems can lead to adult acquired flatfoot deformity (AAFD), a condition that results in a fallen arch with the foot pointed outward. Most people - no matter what the cause of their flatfoot - can be helped with orthotics and braces. In patients who have tried orthotics and braces without any relief, surgery can be a very effective way to help with the pain and deformity. This article provides a brief overview of the problems that can result in AAFD. Further details regarding the most common conditions that cause an acquired flatfoot and their treatment options are provided in separate articles. Links to those articles are provided. 
Causes
The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction. What causes adult acquired flat foot? Fracture or dislocation. Tendon laceration. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Some symptoms of adult acquired flat foot are pain along the inside of the foot and ankle, pain that increases with activity, and difficulty walking for long periods of time. You may experience difficulty standing, pain on the outside of the ankle, and bony bumps on the top of the foot and inside the foot. You may also have numbness and tingling of the feet and toes (may result from large bone spurs putting pressure on nerves), swelling, a large bump on the sole of the foot and/or an ulcer (in diabetic patients). Diabetic patients should wear a properly fitting diabetic shoe wear to prevent these complications from happening.
Diagnosis
Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered.
Non surgical Treatment
In the early stages, simple pre-fabricated orthotics can help improve the heel position to reduce the mechanical load which is contributing to the symptoms. In advanced stages or long term orthotic use, a plaster of paris or foam box cast can be taken and specific bespoke orthotics manufactured. If the condition develops further a AFO (ankle foot orthotic) may be necessary for greater control. In more advanced stages of symptomatic Adult Acquired flat feet, where the conservative methods of treatment have failed there are various forms of surgery available depending upon the root cause of the issue and severity. 
Surgical Treatment
Surgical treatment should be considered when all other conservative treatment has failed. Surgery options for flatfoot reconstruction depend on the severity of the flatfoot. Surgery for a flexible flatfoot deformity (flatfoot without arthritis to the foot joints) involves advancing the posterior tibial tendon under the arch to provide more support and decrease elongation of the tendon as well as addressing the hindfoot eversion with a osteotomy to the calcaneus (surgical cut in the heel bone). Additionally, the Achilles tendon may need to be lengthened because of the compensatory contracture of the Achilles tendon with flatfoot deformity. Flatfoot deformity with arthritic changes to the foot is considered a rigid flatfoot. Correction of a rigid flatfoot deformity usually involves surgical fusion of the hindfoot joints. This is a reconstructive procedure which allows the surgeon to re-position the foot into a normal position. Although the procedure should be considered for advanced PTTD, it has many complications and should be discussed at length with your doctor.
What'S Posterior Tibial Tendon Dysfunction ?
Overview
Have you noticed the arch in your foot collapse over a fairly short period of time as an adult? Or Do you suffer from pain on the inside and sole of your arch? If it does, then you may be suffering from a condition known as adult acquired flat foot. As one of the main support structures of the foot?s arch, the tibilais posterior tendon, along with other muscles, tendons and ligaments, play a very important role in its mechanical function. 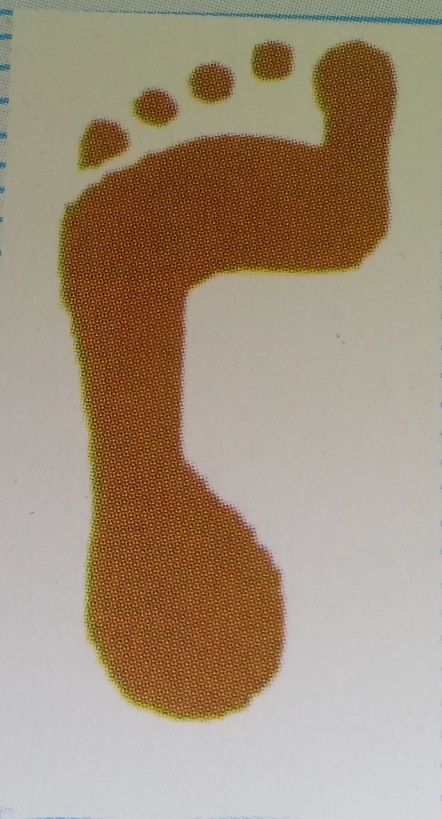
Causes
Many health conditions can create a painful flatfoot, an injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity.
Symptoms
The symptom most often associated with AAF is PTTD, but it is important to see this only as a single step along a broader continuum. The most important function of the PT tendon is to work in synergy with the peroneus longus to stabilize the midtarsal joint (MTJ). When the PT muscle contracts and acts concentrically, it inverts the foot, thereby raising the medial arch. When stretched under tension, acting eccentrically, its function can be seen as a pronation retarder. The integrity of the PT tendon and muscle is crucial to the proper function of the foot, but it is far from the lone actor in maintaining the arch. There is a vital codependence on a host of other muscles and ligaments that when disrupted leads to an almost predictable loss in foot architecture and subsequent pathology.
Diagnosis
Observation by a skilled foot clinician and a hands-on evaluation of the foot and ankle is the most accurate diagnostic technique. Your Dallas foot doctor may have you do a walking examination (the most reliable way to check for the deformity). During walking, the affected foot appears more pronated and deformed. Your podiatrist may do muscle testing to look for strength deficiencies. During a single foot raise test, the foot doctor will ask you to rise up on the tip of your toes while keeping your unaffected foot off the ground. If your posterior tendon has been attenuated or ruptured, you will be unable to lift your heel off the floor. In less severe cases, it is possible to rise onto your toes, but your heel will not invert normally. X-rays are not always helpful as a diagnostic tool for Adult Flatfoot because both feet will generally demonstrate a deformity. MRI (magnetic resonance imaging) may show tendon injury and inflammation, but can?t always be relied on for a complete diagnosis. In most cases, a MRI is not necessary to diagnose a posterior tibial tendon injury. An ultrasound may also be used to confirm the deformity, but is usually not required for an initial diagnosis.
Non surgical Treatment
Patients can be treated non-surgically with in-shoe devices and braces to hold their feet in the correct position. This can reduce pain and damage and assist with walking. Physical therapy is also given to improve muscle strength and help prevent injury to the foot. Surgery can be performed if the patient doesn?t find any relief. 
Surgical Treatment
If initial conservative therapy of posterior tibial tendon insufficiency fails, surgical treatment is considered. Operative treatment of stage 1 disease involves release of the tendon sheath, tenosynovectomy, debridement of the tendon with excision of flap tears, and repair of longitudinal tears. A short-leg walking cast is worn for 3 weeks postoperatively. Teasdall and Johnson reported complete relief of pain in 74% of 14 patients undergoing this treatment regimen for stage 1 disease. Surgical debridement of tenosynovitis in early stages is believed to possibly prevent progression of disease to later stages of dysfunction.